
One of the various devastating moments during LB’s inquest was the revelation that another patient had died in the same bath in 2006. Can you imagine?
As difficult as it is to believe, the same psychiatrist, Dr J, who rang me at work the morning LB died in a pretty lackadaisical way, signed the patient’s death certificate in June 2006. The two 999 calls made the morning LB died were played in court. (The unit phone wasn’t working). I didn’t listen to the first but the second, by Dr J, was extraordinary in that the operator, after three or four minutes of collecting detail, was completely unaware of the urgency of the situation and was going to tick a ‘within four hours’ response box. Can you imagine?
Dr J meanwhile seems to have remained resolutely unreflective about these two events, not mentioning the earlier death in her statement or live evidence and mouthing to me across the court ‘Are you ok?’
At least two other staff members were working in STATT in 2006. No one mentioned this earlier patient in their statement or evidence. Or during the Verita ‘investigation’. No one saw the bath as a potentially risky space. No one seemed to give a shit.
The bare facts: a patient in his 50s had a seizure in the bath (non epileptic seizure though how this was determined is a mystery to me) with someone present who apparently struggled to get him out of the bath. His cause of death is recorded as 1a. convulsion with asphyxiation due to 1b. malnutrition, and 2a. contributing cause depression. There was no postmortem or inquest. The coroner is now investigating whether an inquest should be reopened into his death.
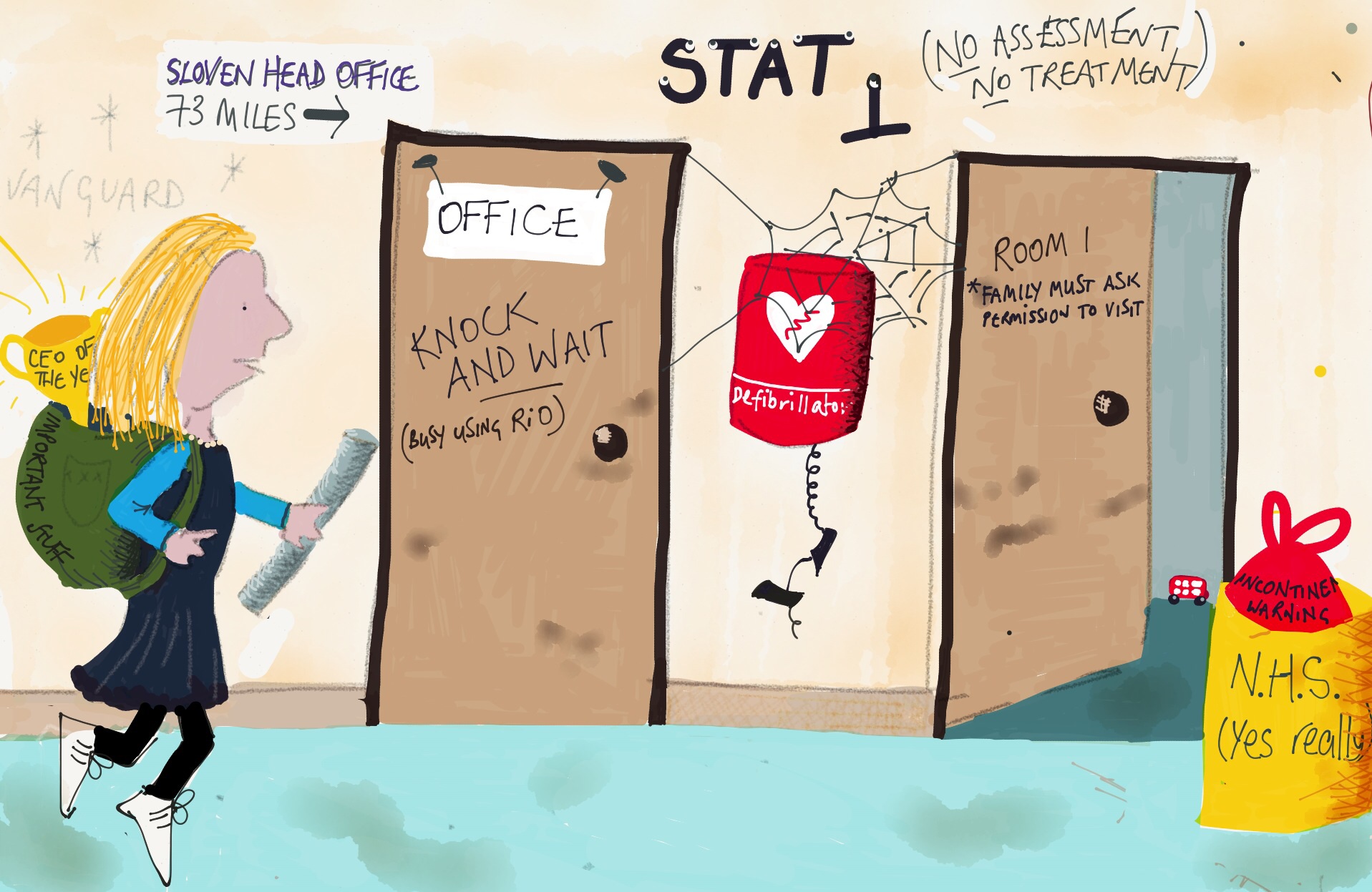
Sloven, of course, come out of this deeply sad tale coated in crapshite. The more recent back story: Back in March 2014, a CQC inspection of a unit on the Slade House site (next to the now closed STATT unit) criticised a bath ban. Dr M, the consultant psychiatrist (who together with her barrister must qualify for some unaward for the pond scummish smear tactics they repeatedly employed during the inquest) apparently vaguely recalled a patient dying back in the day, that the baths were found to be unsafe as they were too deep and after some ‘leadership mentoring’ (always a dangerous thing for those who shouldn’t be within whiff of leadership) banned baths.
This ban, falling foul of the CQC, caused an on the spot investigation on the instruction of Sloven execs. [NB. The same execs who didn’t go near STATT after LB’s death to check the provision was safe for other patients. Death schmeath*. It takes a CQC inspection and hint of bad publicity to get action. Every time]. Once the earlier death came to light, Sloven management apparently actively discouraged Dr M from raising this issue further. She left Sloven’s employment (on what terms?), relinquished her licence in the UK and went back to Ireland to, erm, ‘practice’ there.There was then an apparent burying of this information until the first week of the inquest when it was disclosed by Dr M’s legal representative. Sloven did their best to re-bury it during the inquest by insisting the patient died of cardiac arrest in very different circumstances. Mmm. (Same) bath, seizure, death… I dunno. Strikes me as pretty fucking relevant, at least to be disclosed in order for any relevance to be properly examined.
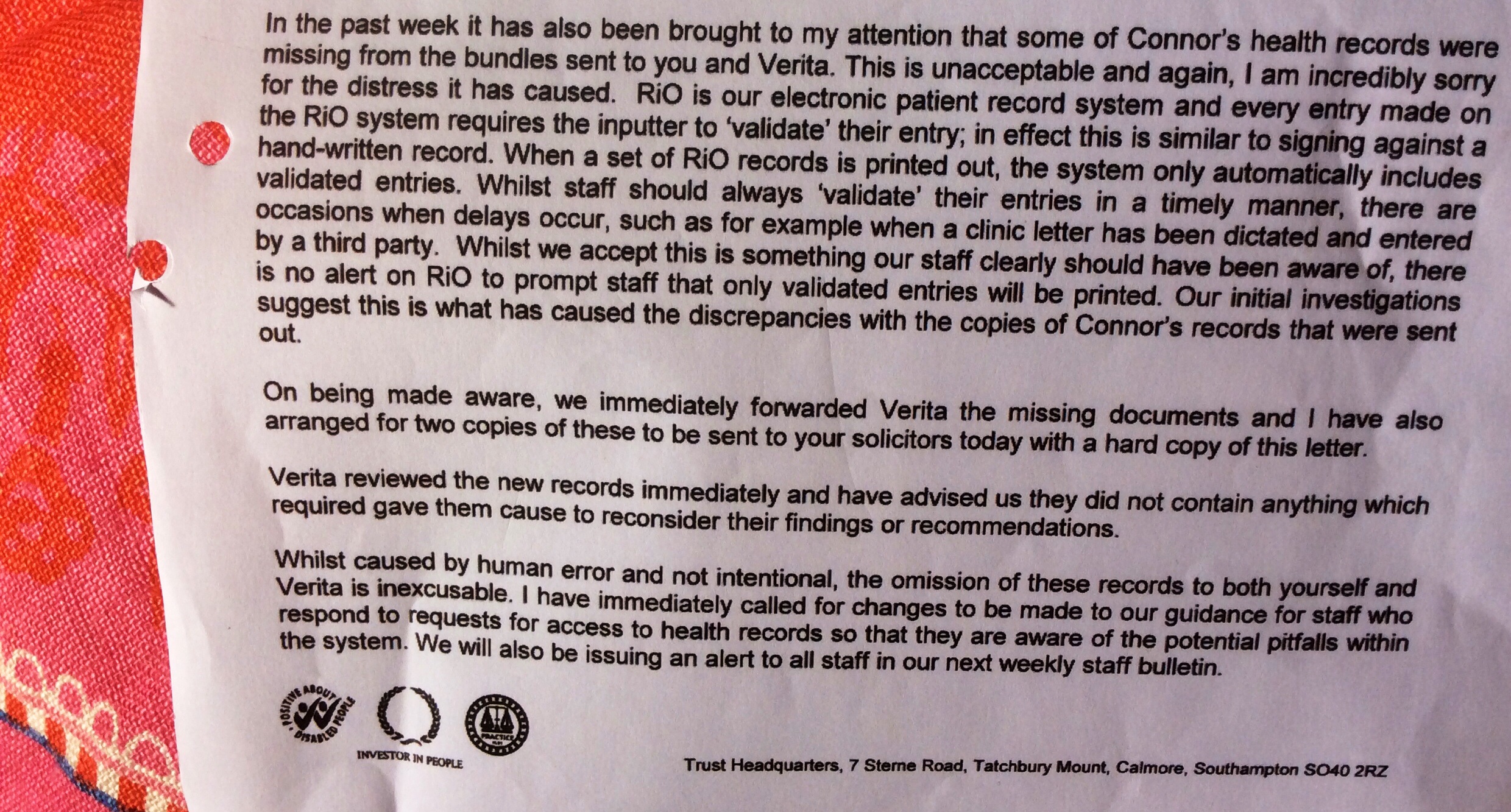
What a sad and sleazy little tale. From a public sector body who claim 100% candour compliance in their 2014/5 annual report. The deliberate concealment of a similar death on the part of Sloven (even to their legal representative) revealed in an obscure and disingenuous way during the inquest. Adding even more (I didn’t think it was possible) distress to a harrowing experience.
We’re left wondering what else hasn’t been disclosed? How often does this level of cover up happen within the NHS? And was there any point to the Francis Inquiry?

*As the Mazar’s death review will reveal, in harrowing detail if it’s ever published.




































{kind=link}